
Guidance for healthcare providers by Doctors Opposing Circumcision and Medical Professionals for Genital Autonomy.

Introduction.
There is much uncertainty among health care workers about when the foreskin of a boy should become retractable.1 This has caused many false diagnoses of phimosis, followed by unnecessary circumcision, when, in fact, the foreskin is developmentally normal.
History.
The first data on development of retractile foreskin were provided in 1949 by the famous British paediatrician, Douglas Gairdner. (2) His data have been incorporated into many textbooks and still is repeated in the medical literature today. Gairdner said that 80 percent of boys should have a retractable foreskin by the age of two years, and 90 percent of boys should have a retractable prepuce by the age of three years. (2) Unfortunately, Gairdner’s data are inaccurate, (3-4) so most healthcare providers have been taught inaccurate data. (4) Retractability usually occurs much later than previously believed. (3) This page provides accurate data, derived from newer and better studies, for healthcare providers.
Current View.
Almost all boys are born with the foreskin fused with the underlying glans penis. Most also have a narrow foreskin that cannot retract. Non-retractile foreskin is normal at birth and remains common until after puberty (age 18). Some boys develop retractile foreskin earlier, and about 2 percent of males have a non-retractile foreskin throughout life. Non-retractile foreskin is not a disease and does not require treatment.
There are three possible conditions that cause non-retractile foreskin:
The first two reasons are normal in childhood and are not pathological in children. The third can be treated conservatively, retaining the foreskin.
Infants and pre-school.
Kayaba et al. (1996) reported that before six months of age, no boy had a retractable prepuce; 16.5 percent of boys aged 3-4 had a fully retractable prepuce. (5) Imamura (1997) examined 4521 infants and young boys. He re-ported that the foreskin is retractile in 3 percent of infants aged one to three months, 19.9 percent of those aged ten to twelve months, and 38.4 percent of three-year-old boys. (6) Ishikawa & Kawakita (2004) reported no retractability at age one, (but increasing to 77 percent at age 11-15). (7) Non-retractile foreskin is the more common condition in this age group. Compare these data with Gairdner’s data!
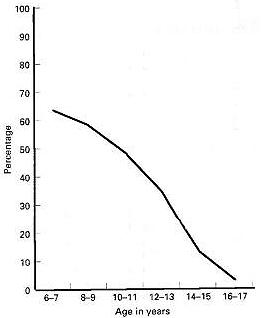
Percentage of boys with fused foreskin by age according to Øster
School-age and adolescence.
Jakob Øster, a Danish physician who conducted school examinations, reported his findings on the examination of school-boys in Denmark, where circumcision is rare.8 Øster (1968) found that the incidence of fusion of the foreskin with the glans penis steadily declines with increasing age and foreskin retractability increases with age.8 Kayaba et al. (1996) also investigated the development of foreskin retraction in boys from age 0 to age 15.5 Kayaba et al. also reported increasing retractability with increasing age. Kayaba et al. reported that about only 42 percent of boys aged 8-10 have fully retractile foreskin, but the percentage increases to 62.9 percent in boys aged 11-15.5 Imamura (1997) reported that 77 percent of boys aged 11-15 had retractile foreskin. (6) Thorvaldsen & Meyhoff (2005) conducted a survey of 4000 young men in Denmark. (9) They report that the mean age of first foreskin retraction is 10.4 years in Denmark. (9) Non-retractile foreskin is the more common condition until about 10-11 years of age.
Percentage of boys with tight ring totally non-retractile foreskin according to Kayaba et al.
Discussion.
Boys usually are born with a non-retractile foreskin. The foreskin gradually becomes retractable over a variable period of time ranging from birth to 18 years or more. (8,9) There is no “right” age for the foreskin to become retractable. Non-retractile foreskin does not threaten health in childhood and no intervention is necessary. Many boys only develop a retractable foreskin after puberty. Education of concerned parents usually is the only action required. (10)
Avoidance of premature retraction.
Care-givers and healthcare providers must be careful to avoid premature retraction of the foreskin, which is contrary to medical recommendations, painful, traumatic, tears the attachment points (synechiae), may cause infection, is likely to generate medico-legal problems, and may cause paraphimosis, with the tight foreskin acting like a tourniquet. The first person to retract the boy’s foreskin should be the boy himself. (3)
Making the foreskin retractable.
Occasionally a male reaches adulthood with a non-retractile foreskin. Some men with a non-retractile foreskin happily go through life and father children. Other men, however, may want to make their foreskin retractile.
The foreskin can be made retractable by:
Male circumcision is outmoded as a treatment for non-retractile foreskin, but it is still recommended by many urologists because of lack of adequate information, and perhaps because of the fees associated with circumcision. Nevertheless, circumcision should be avoided because of pain, trauma, cost, (15,16) complications, (15) difficult recovery, permanent injury to the appearance of the penis, loss of pleasurable erogenous sensation, (17) and impairment of erectile and ejaculatory functions. (18-20)
A website exists here where knowledable individuals give free advice to adults and teens on stretching one's foreskin to make it retractble.
References:


Photo by David Burnett
Introduction.
There is much uncertainty among health care workers about when the foreskin of a boy should become retractable.1 This has caused many false diagnoses of phimosis, followed by unnecessary circumcision, when, in fact, the foreskin is developmentally normal.
History.
The first data on development of retractile foreskin were provided in 1949 by the famous British paediatrician, Douglas Gairdner. (2) His data have been incorporated into many textbooks and still is repeated in the medical literature today. Gairdner said that 80 percent of boys should have a retractable foreskin by the age of two years, and 90 percent of boys should have a retractable prepuce by the age of three years. (2) Unfortunately, Gairdner’s data are inaccurate, (3-4) so most healthcare providers have been taught inaccurate data. (4) Retractability usually occurs much later than previously believed. (3) This page provides accurate data, derived from newer and better studies, for healthcare providers.
Current View.
Almost all boys are born with the foreskin fused with the underlying glans penis. Most also have a narrow foreskin that cannot retract. Non-retractile foreskin is normal at birth and remains common until after puberty (age 18). Some boys develop retractile foreskin earlier, and about 2 percent of males have a non-retractile foreskin throughout life. Non-retractile foreskin is not a disease and does not require treatment.
There are three possible conditions that cause non-retractile foreskin:
- Fusion of the foreskin with the glans penis
- Tightness of the foreskin orifice
- Frenulum breve (which is rare and cannot be diagnosed until the previous two reasons have been eliminated)
The first two reasons are normal in childhood and are not pathological in children. The third can be treated conservatively, retaining the foreskin.
Infants and pre-school.
Kayaba et al. (1996) reported that before six months of age, no boy had a retractable prepuce; 16.5 percent of boys aged 3-4 had a fully retractable prepuce. (5) Imamura (1997) examined 4521 infants and young boys. He re-ported that the foreskin is retractile in 3 percent of infants aged one to three months, 19.9 percent of those aged ten to twelve months, and 38.4 percent of three-year-old boys. (6) Ishikawa & Kawakita (2004) reported no retractability at age one, (but increasing to 77 percent at age 11-15). (7) Non-retractile foreskin is the more common condition in this age group. Compare these data with Gairdner’s data!
Percentage of boys with fused foreskin by age according to Øster
School-age and adolescence.
Jakob Øster, a Danish physician who conducted school examinations, reported his findings on the examination of school-boys in Denmark, where circumcision is rare.8 Øster (1968) found that the incidence of fusion of the foreskin with the glans penis steadily declines with increasing age and foreskin retractability increases with age.8 Kayaba et al. (1996) also investigated the development of foreskin retraction in boys from age 0 to age 15.5 Kayaba et al. also reported increasing retractability with increasing age. Kayaba et al. reported that about only 42 percent of boys aged 8-10 have fully retractile foreskin, but the percentage increases to 62.9 percent in boys aged 11-15.5 Imamura (1997) reported that 77 percent of boys aged 11-15 had retractile foreskin. (6) Thorvaldsen & Meyhoff (2005) conducted a survey of 4000 young men in Denmark. (9) They report that the mean age of first foreskin retraction is 10.4 years in Denmark. (9) Non-retractile foreskin is the more common condition until about 10-11 years of age.
Percentage of boys with tight ring totally non-retractile foreskin according to Kayaba et al.
Discussion.
Boys usually are born with a non-retractile foreskin. The foreskin gradually becomes retractable over a variable period of time ranging from birth to 18 years or more. (8,9) There is no “right” age for the foreskin to become retractable. Non-retractile foreskin does not threaten health in childhood and no intervention is necessary. Many boys only develop a retractable foreskin after puberty. Education of concerned parents usually is the only action required. (10)
Avoidance of premature retraction.
Care-givers and healthcare providers must be careful to avoid premature retraction of the foreskin, which is contrary to medical recommendations, painful, traumatic, tears the attachment points (synechiae), may cause infection, is likely to generate medico-legal problems, and may cause paraphimosis, with the tight foreskin acting like a tourniquet. The first person to retract the boy’s foreskin should be the boy himself. (3)
Making the foreskin retractable.
Occasionally a male reaches adulthood with a non-retractile foreskin. Some men with a non-retractile foreskin happily go through life and father children. Other men, however, may want to make their foreskin retractile.
The foreskin can be made retractable by:
- Manual stretching (11-12)
- Application of topical steroid ointment (13-14)
Male circumcision is outmoded as a treatment for non-retractile foreskin, but it is still recommended by many urologists because of lack of adequate information, and perhaps because of the fees associated with circumcision. Nevertheless, circumcision should be avoided because of pain, trauma, cost, (15,16) complications, (15) difficult recovery, permanent injury to the appearance of the penis, loss of pleasurable erogenous sensation, (17) and impairment of erectile and ejaculatory functions. (18-20)
A website exists here where knowledable individuals give free advice to adults and teens on stretching one's foreskin to make it retractble.
References:
- Simpson ET, Barraclough P. The management of the paediatric foreskin. Aust Fam Physician 1998;27(5):381-3. [Full Text]
- Gairdner D. The fate of the foreskin: a study of circumcision. Br Med J 1949;2:1433-7. [Full Text]
- Wright JE. Further to the "Further Fate of the Foreskin." Med J Aust 1994;160:134-5. [Full Text]
- Hill G. Circumcision for phimosis and other medical indications in Western Australian boys. Med J Aust 2003;178(11):587. [Full Text]
- Kayaba H, Tamura H, Kitajima S, et al. Analysis of shape and retractability of the prepuce in 603 Japanese boys. J Urol 1996;156(5):1813-5. [Full Text]
- Imamura E. Phimosis of infants and young children in Japan. Acta Paediatr Jpn 1997;39(4):403-5. [Abstract]
- Ishikawa E, Kawakita M. [Preputial development in Japanese boys]. Hinyokika Kiyo 2004;50(5):305-8. [Abstract]
- Øster J. Further fate of the foreskin: incidence of preputial adhesions, phimosis, and smegma among Danish schoolboys. Arch Dis Child 1968;43:200-3. [Full Text]
- Thorvaldsen MA, Meyhoff H. Patologisk eller fysiologisk fimose? Ugeskr Læger 2005;167(17):1858-62. [Full Text]
- Spilsbury K, Semmens JB, Wisniewski ZS. et al. Circumcision for phimosis and other medical indications in Western Australian boys. Med J Aust 2003 178 (4):155-8. [Full Text]
- Dunn HP. Non-surgical management of phimosis. Aust N Z J Surg 1989;59(12):963. [Full Text]
- Beaugé M. The causes of adolescent phimosis. Br J Sex Med 1997; Sept/Oct: 26. [Full Text]
- Orsola A, Caffaratti J, Garat JM. Conservative treatment of phimosis in children using a topical steroid. Urology 2000;56(2):307-10. [Full Text]
- Ashfield JE, Nickel KR, Siemens DR, et al. Treatment of phimosis with topical steroids in 194 children. J Urol 2003;169(3):1106-8. [Abstract]
- Van Howe RS. Cost-effective treatment of phimosis. Pediatrics 1998; 102(4)/e43. [Full Text]
- Berdeu D, Sauze L, Ha-Vinh P. Blum-Boisgard C. Cost-effectiveness analysis of treatments for phimosis: a comparison of surgical and medicinal approaches and their economic effect. BJU Int2001;87(3):239-44. [Full Text]
- Williams N, Kapila L. Complications of circumcision. Brit J Surg 1993;80:1231-6. [Full Text]
- Denniston GC, Hill G. Circumcision in adults: effect on sexual function. Urology 2004;64(6);1267. [Full Text]
- Shen Z, Chen S, Zhu C, et al. [Erectile function evaluation after adult circumcision]. Zhonghua Nan Ke Xue 2004;10(1):18-9. [Abstract]
- Masood S, Patel HRH, Himpson RC, et al. Penile sensitivity and sexual satisfaction after circumcision: Are we informing men correctly? Urol Int 2005;75(1):62-5. [Full Text]
Related Reading on Intact Care:
 |
| How to care for your son if he is retracting pre-puberty. |
 |
| Foreskin Facts postcards available at Etsy |






